



What is ambulatory surgery / same-day-surgery?
Ambulatory typically means “the ability to walk” but in the context of surgery, it refers to patients who are able to leave the hospital the same day as the surgery, without being admitted to the hospital. Ambulatory surgery is referred to by other names, commonly called minimally invasive surgery, outpatient surgery or same-day surgery. When you hear someone refer to same-day surgery, they mean an ambulatory procedure.
Traditionally spine surgery used to be intense and required long hospital stay and longer recovery time. In the past decade, there has been a major shift toward performing spine surgery in an outpatient setting . Thirty years ago, almost all surgeries were performed at a hospital on people who had been admitted as patients.
Over time, however, techniques have evolved, and safety concerns have been addressed. Now, health experts predict that 50 percent of all spine surgeries will be performed on an outpatient basis within the next five years.
What has changed?
1.Evolution of techniques in the field of spine surgery
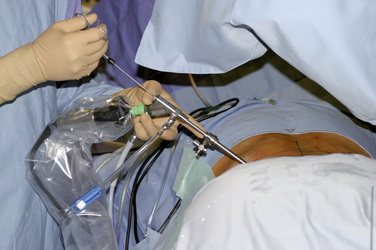
Minimally invasive surgery-There has been more and more minimally invasive surgery being performed. It reduces tissue trauma and pain and accelerates recovery. Techniques like microdiscectomy, minimally invasive discectomy and percutaneous endoscopic techniques have been a game changer, driving day surgery possible. Techniques like XLIF, MIS ALIF, MIS TLIF,OLIF has also made lumbar fusion surgery an ambulatory surgery.

2.Technological advances in the field of navigation/ robotics
Minimally invasive surgeries are further made safe by using navigation techniques.It helps in reducing the size of the wound and providing high accuracy and safety. Complex surgeries are made possible with higher safety standards with these techniques. With evolving technology like robotic surgery and VR technology , we can further see seabchanges in day surgery setting.

3.Advanced Anaesthetic Techniques
With advances in every field of surgery, its no surprise that anaesthetic techniques have evolved to accommodate the need for surgeon and patient alike. Careful preop preparation of patient, pre op medications, reducing the need for post op strong opioids and carbohydrate loading preop are few of the techniques anaesthetist uses to supplement day surgeries.
Techniques like epidural analgesia for spine surgery, para spinal blocks and local anaesthesia with liposomal bupivacaine ( 72 hours ) have contributed to driving the spine day surgery programmes.It has also helped in reducing opioid usage for post-operative pain relief and reduces opioid dependence.


Am I a candidate for ambulatory spine surgery ?
Identifying people who are good candidates for outpatient surgery involves many factors. Most basically, the cause of the condition would be well defined, and the patient would have seen no improvement despite a reasonable amount of nonsurgical care. Then comes the nature of spine surgery. Not all spine surgeries are amenable as day surgery.
If those conditions are met, the ideal candidate:
- Has no other medical conditions
- Is of normal weight (body mass index, or BMI, less than 35)
- Has sufficient family or social support at home
- Has a realistic expectation of some pain and discomfort despite reasonable pain-relief strategies
- Easy access to health care facility within 30 minutes time period
- Not everyone is this ideal candidate, and each additional risk factor must be weighed before offering outpatient spine surgery.

What are the spine surgeries that are possible to be done as day surgeries?
Lumbar discectomy
The first type of spine surgery that became commonly performed as an outpatient procedure is the lumbar discectomy. This surgery is performed to remove the herniated portion of the lumbar disc. It has a high success rate, especially in relieving leg pain (or sciatica), caused by the herniated portion of the disc pressing against a nerve.
Traditionally discectomy used to be done open several decades ago. With evolution of techniques to micro discectomy , tubular discectomy and percutaneous endoscopic discectomy day surgery discectomy has become common place.
In addition these mis techniques reduces the size of scar accelerates recovery and less time off from work as compared to previous days.


Due to minimal dissection of the muscles and other soft tissues, post-operative pain is tolerable. By removing the portion of the disc that is irritating the nerve, usually the pre-operative radiculopathy pain has diminished or resolved, and many patients feel immediate improvement in their leg pain when they wake up from the surgery.
Typically, patients will leave the recovery room, and go home, with less pain than they had before the surgery.
For the carefully selected patient, outpatient lumbar discectomy has become a routine surgical choice with highly predictable success rates.
https://www.myspineworld.com/discectomy-conventional-to-state-of-the-art/
Above procedures are commonly done on an outpatient basis; an overnight hospital stay would only be required if there are special considerations, such as the patient’s medical condition or complicating factors, or if for some reason the patient would not be able to recover at home or in a place outside of a hospital.
Lumbar laminectomy
In lumbar spinal stenosis, compression of the spinal nerve roots in the lower back can cause pain. If the symptomatic stenosis area localizes to a few spots, modern minimally invasive spinal surgery techniques can be used to perform a focused decompression of the specific areas of stenosis.
Again, traditional laminectomy and decompression used to be done with open methods
With advancing technological measures it can be done using microscopic techniques, tubular techniques and also endoscopic techniques. With endoscopic technique, which is the least minimally invasive of all the above, the wound is less than a cm long with minimal muscle dissection and minimal pain.

Outpatient lumbar decompression techniques reduce the surgical exposure, while achieving the removal of the spinal stenosis-causing structures. For the carefully selected patient, there is a high level of satisfaction, with minimal added risk with the outpatient process
Cervical laminotomy/ discectomy
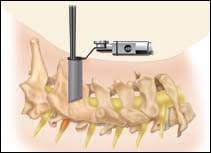
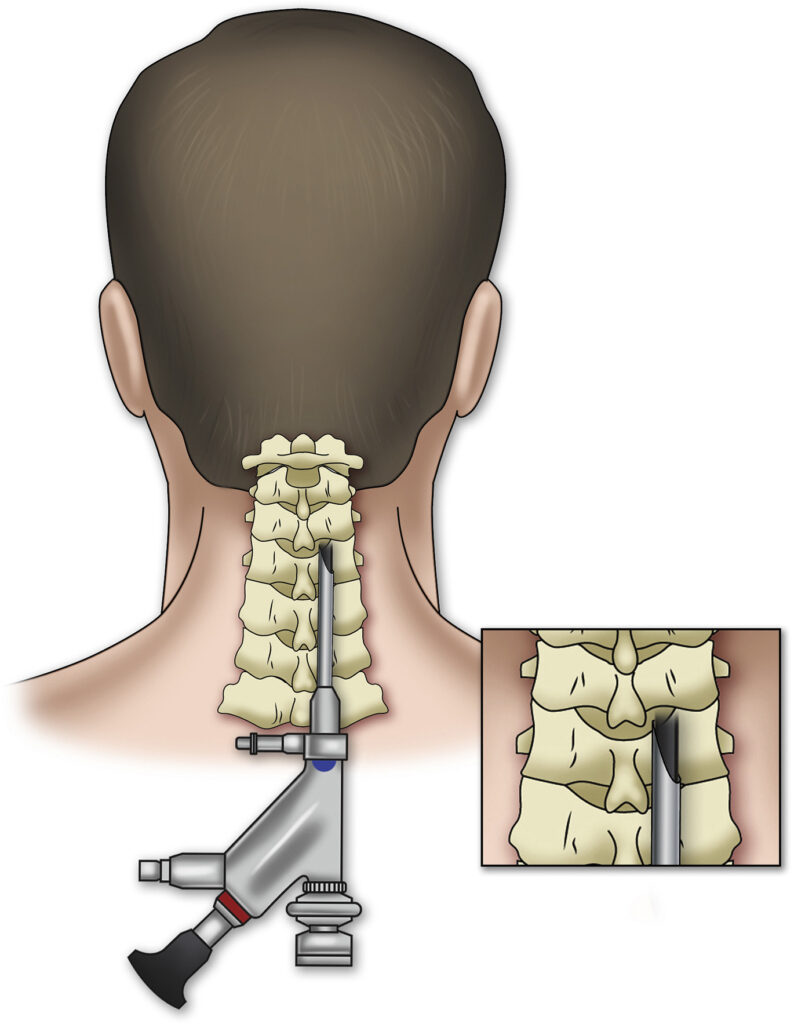
Similar to outpatient lumbar discectomy and laminotomy, approaches to a late raly located (to the side) cervical disc herniation or foraminal narrowing utilizes the same technique. Fluoroscopic guidance minimizes the incision, and tissue-splitting techniques reduce the impact to the muscles and ligaments of the spine. Magnification techniques and specialized tools can allow for a precise removal of the offending bone, tissue, or disc.
This surgery can be done these days with tubular retractors and even with endoscopic technique, thus reducing the incision further and making recovery faster.
However all cervical discectomy may not be possible with this technique
- In the cervical spine, the disc herniation should be located to the side (laterally), or near the foramen (the gap in vertebrae in the back and to the side of the spine). With this location, there is no need for any significant retraction on the spinal cord.
- If the disc is more centrally located, meaning it has herniated toward the back of the spine and is impinging on the spinal cord, the risk associated with moving the cord away from the disc is high. Most surgeons would consider another surgical approach that allows greater visualization, rather than risk causing spinal cord injury.
- As the spinal cord travels down the spine, it branches out into individual nerves and exits the spinal canal, so it does not run through the lumbar spine. The branching allows individual nerves to be retracted in the lumbar spine without concern for any spinal cord damage. Therefore, for most types of disc herniations in the lumbar spine, retraction of the nerve sac is much more acceptable and tolerated in lumbar procedures.
Cervical and lumbar fusion surgeries
Cervical fusion
At one time, there was significant concern about potential post-operative complications associated with this technique. Several studies have documented the efficacy and safety of ACDF ( anterior cervical discectomy and fusion )and in the outpatient setting, however.
See Potential Risks and Complications of ACDF Surgery
While the ACDF technique has multiple steps, there is minimal dissection of the tissues.
- The incision is typically 1 to 2 inches long
- After the incision to the front of the neck, the rest of the dissection is performed bluntly, with no more cutting
- The muscles and tissues are gently pushed away from the front of the spine bone
- There is usually minimal blood loss, and the targeted discs are readily identified and visualized


Because the dissection is performed in a tissue-splitting instead of tissue-cutting fashion, the postoperative neck pain is tolerable. With resolution of the pre-operative arm radiculopathy symptoms in the recovery area, many will experience less pain than immediately before the operation. (Radiculopathy is pain caused by irritation of a spinal nerve root.)
As long as the patient can tolerate the pain and there is no concern about breathing issues or with difficulty swallowing (dysphagia), most patients can go home from the recovery area within a few hours of the surgery.
Within the past few years, cervical disc replacement procedures have also been performed on an outpatient basis. Using the same exposure techniques, there is no difference in terms of immediate postoperative pain from the ACDF surgery.
Lumbar Fusion
The past 15 years, advances in spine surgery instrumentation have yielded a tremendous selection of percutaneously delivered spine screws, cages, and exposure retractors. These instruments are designed to create a lumbar spine fusion construct that can be delivered using small incisions and muscle-splitting dissections.
However the type of fusion surgery will be selected and the appropriateness of day surgery has to be selected based on a variety of factors and hence may not be suited for many patients.
Specific fusion surgeries like MIS -TLIF , MIS ALIF,XLIF,OLIF surgeries may be considered to be done in outpatient setting.
However as the lumbar spine has more musculature involved in dissection, pain score will be slightly more compared to cervical fusion surgeries, especially with posterior approaches. However with newer techniques like endoscopic fusion surgery even posterior approach can be considered for ambulatory surgery.
Game changer ?
As technology evolves more and more spine surgeries will be done as day surgeries. This change has been in response to decreasing invasiveness of surgery, patients’ desire to recuperate at home, and significant net reductions in cost, which is critical in this era of value-based care. However, it applies to a selected group of patients with careful selection criteria and strict postoperative protocols in place.
These “techniques” in effect provide a larger body of “tools” in the armamentarium that is available to the spinal surgeon these days to address the patients’ pathology.
The utility of the “tool” is highly dependent on the skills and preferences of the artisan with respect to the use of the tool and his or her ability to deliver the intended results based on their mastery of the tools.
As always, surgery will remain an art as well as a science with its greatest accomplishment, perhaps being able to know when not to operate apart from knowing how to operate and who to operate upon.
Take guidance from your doctor/ surgeon and see you soon with some more spine tips in My Spine World. Remember, we got your back!